Mass Vaccinator Jobs
5 September 2021
So the Joint Committee on Vaccination and Immunisation (JCVI) states that their “Current Advice” on COVID-19 “vaccinations” according to the latest statement from them published on the 4th August 2021 advises “COVID-19 vaccination of all adults aged 18 years and over in the UK, and vaccination of some specific groups under the age of 18 years”, which we know.
They immediately make the claim that…
The COVID-19 immunisation programme has been highly successful, with rapid delivery and high uptake. The programme has already substantially reduced the risk from severe COVID-19 in the UK population and is estimated to have averted approximately 22 million infections and 60,000 deaths to date.
https://www.gov.uk/government/publications/jcvi-statement-august-2021-covid-19-vaccination-of-children-and-young-people-aged-12-to-17-years/jcvi-statement-on-covid-19-vaccination-of-children-and-young-people-aged-12-to-17-years-4-august-2021
The estimation of averting 22 million infections and 60,000 deaths is a link. That implies the link would take you to evidence to support the accuracy of this claim. It doesn’t. It takes you to the “COVID-19 vaccine surveillance reports” page, a list of documents containing the weekly surveillance reports, where you are presumably meant to open the latest and wade through the 25 pages to find the evidence. If you did that, you wouldn’t find any evidence or references to support this claim at all.
You might read through and get to page 17 and a section titled “Direct impact on hospitalisations”, where it says…
The number of hospitalisations averted by vaccination, can be estimated by considering vaccine effectiveness against hospitalisation, vaccine coverage and observed hospitalisations and through modelling using a range of parameters.
Page 17 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1014788/Vaccine_surveillance_report_-_week_35.pdf
For the week 35 report the vaccine effectiveness estimates used in the model were updated to use more recent vaccine effective estimates. The vaccine effectiveness estimates used in previous reports were slightly lower than the current estimates, therefore an increase in the number of hospitalisations averted was seen in the week 35
report compared to previous reports.
PHE estimates to 22 August 2021 based on the direct effect of vaccination and vaccine coverage rates, are that around 143,600 hospitalisations have been prevented in those aged 65 years and over in England (approximately 36,100 admissions in those aged 65 to 74, 58,800 in those aged 75 to 84, and 48,700 in those aged 85 and over) as a result of the vaccination programme. There is increasing evidence that vaccines prevent infection and transmission. The indirect effects of the vaccination programme will not be incorporated in this analysis, therefore the figure of 143,600 hospitalisations averted is likely to be an underestimate.
So “vaccine effectiveness estimates” are used in a “model” to project the “number of hospitalisations averted”. Estimates based on what? Well it doesn’t say of course, because they are literally just that, estimates, i.e. “we’d like the effectiveness to be X, so we’ll say it’s X”. This is not evidence in any reasonable understanding of the word, regardless of the laughable claim that “there is increasing evidence that vaccines prevent infection and transmission” because there just isn’t.
If I was to knock on your door and try to sell you a special roof protection coating for your house, because I claimed that raindrops were going to get heavier and smash all your roof tiles, you might ask me for evidence to back up that claim. If I said I had a computer model and then showed you this…
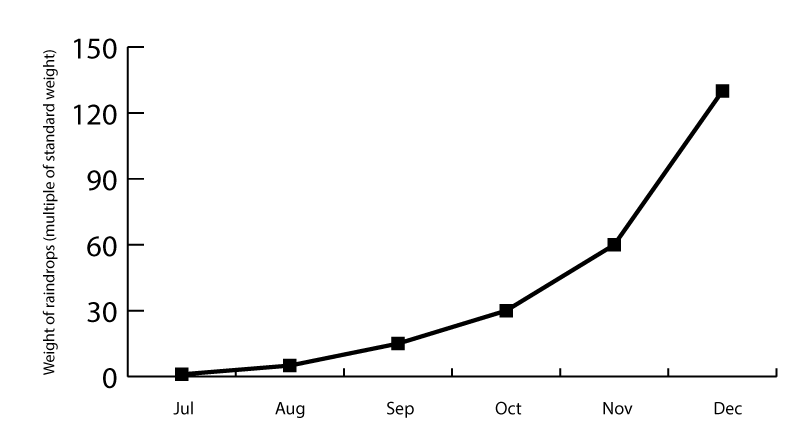
…and after looking at this graph projecting the rise in weight of raindrops over a 6 month period from it’s standard weight in July to 130 times the standard weight by December, you might ask me where I got those numbers from. If I then explained to you that they were estimates I had no actual evidence of, but I had Government paid scientists who had provided the estimates also with no actual evidence, but they had assured me that if anything those figures were an underestimate, I’m fairly sure I’d make a sale there and then, right?
Ah but the vaccine effectiveness estimates are based on clinical trial data, and that’s Science so it’s not like they’re pulling random figures out of orifices now is it? In a previous article titled “Bias in Efficacy Reporting for mRNA Vaccines” we demonstrated with the aid of some proper science and a look at the methods employed to generate those “efficacy” figures how unreliable and open to statistical manipulation they are. Those figures if indeed that is what they are using as they don’t actually say, are not remotely reliable or representative of real-world effectiveness.
Back to the JCVI statement. They have a section on “Vaccine Safety” where they describe the most frequent adverse reactions in persons aged 12 to 17 years are “injection site pain, fever and headache. These reactions are generally mild, self-limiting and short-lived, typically lasting 1 to 2 days” with a little footnote link. That footnote link takes you to the footnote itself, which is intended to be a citation. Usually these are links, but for most of the citations in this document they are not links, so you have to go and search for the publication, or they are listed as “unpublished”. Super helpful. Almost like they don’t really want you to check the “evidence”.
One of the citations is an article on the US National Institutes of Health website titled “Myocarditis following COVID-19 mRNA vaccination” published online in May 2021. This is cited by the JCVI statement as they state that…
In recent weeks, reports have been submitted in the UK and other countries of the extremely rare occurrence of myocarditis (inflammation of the heart muscle) and pericarditis (inflammation of the membrane around the heart), following the use of Pfizer-BioNTech BNT162b2 and Moderna mRNA-1273 vaccines. These extremely rare adverse reactions have been more frequent shortly after the second dose, and in younger individuals and males.
Hmmm, “extremely rare occurrence of myocarditis”. Looking at the article cited they describe how in “a three-week interval (January 30th through February 20th 2021, six men were hospitalized with suspected myocarditis, all shortly after the vaccination”, median age of 22 and otherwise healthy. It would appear this was all at one hospital as the article states:
All six patients presented in less than a month period. We investigated the background rate of myocarditis during winter months (December through March) in our hospital in the past 5 years, and found a mean of 1.17 cases of myocarditis per month
…and:
This finding raises concern that we identified only the “tip of the icberg” i.e. symptomatic cases and other asymptomatic cases may had not been detected.
Of course, the doctors at this hospital and the authors of this article want to keep their jobs, so they conclude with:
It is important to interpret our data with caution because public acceptance of COVID-19 vaccines is much needed. The individual and public benefit from COVID-19 vaccination outweighs these rare findings described herein.
They have done their job insofar as reporting this ~6 times higher than normal prevalence of myocarditis, and that in healthy young men, but care more about the “public acceptance” of the jabs, and after presenting actual scientific evidence regarding the hospitalisation of these young men, and acknowledging this is likely an underrepresentation of the issue, they end with an entirely unscientific claim, parroting the line fed to them by their paymasters i.e. pharmaceutical companies and the Government.
Back to the JCVI statement again. Of course in a statement about if experimenting on children with mRNA genetic therapy is safe there is a section about the “Benefits of vaccination”. It starts with the sentence
“COVID-19 disease in children is typically mild or asymptomatic.”
In other words, it’s like a cold, or they’re not ill at all. The next paragraph starts with
“The incidence of severe outcomes from COVID-19 in children and young people is very low.”
Yes, we know. They also state
“In England, between February 2020 and March 2021 inclusive, fewer than 30 persons aged less than 18 years died because of COVID-19, corresponding to a mortality rate of 2 deaths per million.”
So why is this even up for debate? Why on earth is the idea of giving children an experimental “vaccine” that WILL cause harm being considered when by their own admission less than 30 under 18s have died “because of COVID-19”?
What is even more absurd is the next statement, after admitting less than 30 under 18s have died from COVID-19 (according to them) which is that:
Children and young people at higher risk of severe COVID-19 include those with severe neuro-disabilities, Down’s Syndrome, underlying conditions resulting in immunosuppression, profound and multiple learning disabilities (PMLD), severe learning disabilities or who are on the learning disability register.
Based on what? They claim that the data source for this is from OpenSAFELY but all that does is take you to the OpenSAFELY website home page. It gets more nonsensical as we go on, as the next paragraph claims that:
Efficacy of the Pfizer-BNT162b2 vaccine against symptomatic COVID-19 was 100% in the clinical trial involving persons aged 12 to 15 years. The trial was too small to assess the efficacy against severe COVID-19 in 12 to 15 year olds.
That statement has a footnote reference that is a citation of an article on the New England Journal of Medicine website titled “Safety, Immunogenicity, and Efficacy of the BNT162b2 Covid-19 Vaccine in Adolescents” published in July 2021.
The utterly ridiculous nature of this study is revealed quite clearly in the “results” section. It says that “2260 adolescents 12 to 15 years of age received injections; 1131 received BNT162b2, and 1129 received placebo” and that…
Among participants without evidence of previous SARS-CoV-2 infection, no Covid-19 cases with an onset of 7 or more days after dose 2 were noted among BNT162b2 recipients, and 16 cases occurred among placebo recipients. The observed vaccine efficacy was 100% (95% CI, 75.3 to 100).
https://www.nejm.org/doi/full/10.1056/NEJMoa2107456
Think about what is being said there. Out of the two groups of 12 to 15 years of age “participants” (who is putting their children forward for these trials?) there are some very specific dependencies stated.
Firstly, the number equating to “among participants without evidence of previous SARS-CoV-2 infection” is not stated. Next is “no Covid-19 cases with an onset of 7 or more days after dose 2”, which means there could be cases at 6 days, or after 7 days of the first dose. Out of 1131 in the group that got the BNT162b2 dose, those two specifications could reduce that number to zero. I’m not claiming it did, but it could have as doesn’t specify any numbers. Then we have the “16 cases” that supposedly “occurred among placebo recipients”. Cases. We know that a “case” can simply be a positive PCR test that isn’t a diagnostic test.
Oh, and this “study” was funded and supported by BioNTech and Pfizer, naturally. From this garbage pseudoscience we’re expected to believe the Pfizer/BioNTech mRNA injection is “100% effective”.
Once again, back to the JCVI statement. They remind us that they do advise…
persons aged 12 to 15 years with specific underlying health conditions that put them at risk of severe COVID-19, should be offered 2 doses of Pfizer-BNT162b2 vaccine with an interval of 8 weeks between doses. This currently includes children with severe neuro-disabilities, Down’s Syndrome, underlying conditions resulting in immunosuppression, profound and multiple learning disabilities (PMLD), severe learning disabilities or who are on the learning disability register.
It bears repeating that there clearly is no evidence that children with neuro-disabilities, Down’s Syndrome or learning difficulties are at any statistical higher risk from a respiratory disease. They keep saying it, but never provide any evidence for it, and their own statement that in over 12 months less than 30 under 18s have allegedly died from COVID-19 proves that they are not. But they want them to have the experimental mRNA stuff anyway.
They also say…
Children and young people aged 12 years and over who are household contacts of persons (adults or children) who are immunosuppressed should be offered 2 doses of Pfizer-BNT162b2 vaccine on the understanding that the main benefits from vaccination are related to the potential for indirect protection of their household contact who is immunosuppressed. The offer of vaccination may help to alleviate stress and anxiety experienced by the children and young people living in these difficult circumstances.
The notion that offering the “vaccination” to children who are living with others who are immunosuppressed “may help to alleviate stress and anxiety experienced” is a disgraceful thing to say, when the predatory marketing of this experimental jackpot winner for Pfizer has been based on telling children that they are a threat to adults, that they are going to kill their grandparents and they need to take a demonstrably risky and dangerous experimental gene therapy with no provable benefits to them because of a claimed “potential for indirect protection of their household”.
We are supposed to also believe that the JCVI is still evaluating giving healthy 12-15 year olds this dangerous injection as they ponder the data. This is clearly to create the illusion that they are somehow “following the science” and even though the Government (of which the JCVI is a part) is pushing hard for it, along with people like Devi Sridhar quoted in the Independent as saying…
I think the issue is they are being very cautious. They’re waiting and watching and I guess the issue with a pandemic is that waiting and watching costs time. And time is the currency now that matters because it’s not like we can wait and watch and in six months say ‘OK, it’s safe, let’s vaccinate’. In those six months if a large percentage of 12- to 15-year-olds get infected, in some ways they’ve lost that window of time and so I think perhaps they don’t feel the urgency that they should be feeling given it’s an emergency situation and we have Delta, which is so infectious. I mean, it’s just flying through schools as we know.
Devi Sridhar – https://www.independent.co.uk/news/health/nhs-covid-vaccine-uk-12-years-b1909002.html
It’s “flying through schools” is it? It’s an “emergency situation” is it? There is no-one who’s lived experience in the real-world backs those claims up though. But regardless, the State machinery is gearing up to inject 12-15 year-olds anyway.
In case you are unaware of who Devi Sridhar is, she wrote a book titled “Governing Global Health: Who Runs the World and Why?” with Chelsea Clinton. She is an Associate Fellow with the Chatham House Centre on Global Health. In 2011, she was appointed to Wolfson College, Oxford as an Associate Professor in global health politics. She also serves on the World Economic Forum Global Agenda Council on the Health Industry. Are you seeing the theme yet?
Sridhar is an intelligent woman, and she knows how to position herself in just the right place to sound mostly reasonable. She envelopes her globalist evangelism in the soft embrace of caring about health and poor people, about children and talk of transparency. When you actually look at what she advocates for, not only is it clear it’s not really about the things her talking points appear to be about, but she doesn’t care about public health, children or poor people. When the policies you argue for, however softly and whimsically, are causing more harm than the good they pretend to do, the undeniable evidence is that you don’t care about the colossal damage and lives lost that your policies have directly caused.
While this circus show of a “debate” rages on, the NHS is posting job adverts for “Mass Vaccinators” on job websites like Monster. The attention to detail in the advert in that link is just staggering.
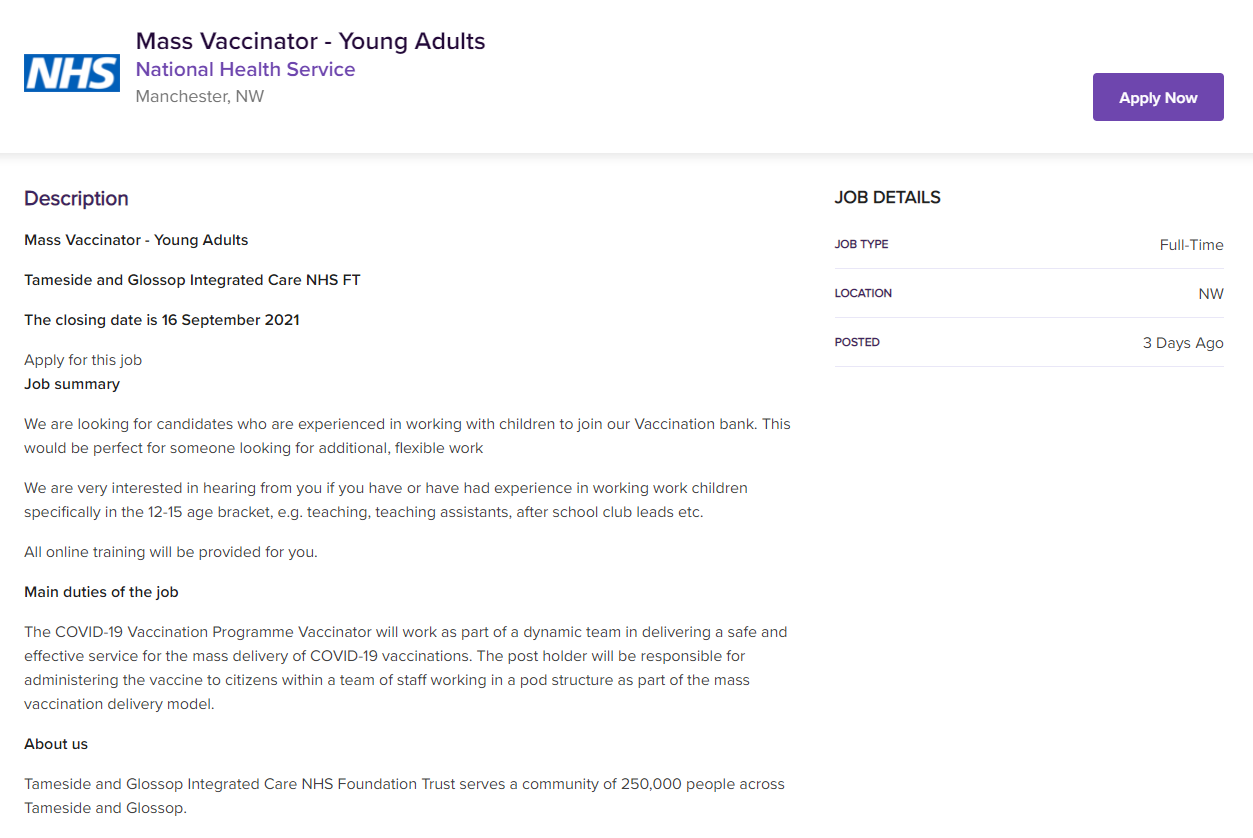
Rest assured this is going to go ahead if the Government has any say in the matter, which of course they do. They are going to give “online training” to teaching assistants and after-school club leads to become Mass Vaccinators in the 12-15 age bracket. Do you think it will stop there?