Long COVID – Is It Mostly Imaginary?
16 November 2021
One of the most overhyped aspects of the fake pandemic has been “Long COVID”. Even if you are able to get people to accept that mild respiratory aliments that occur more in the winter than summer have been something humanity has dealt with for millennia, and this one is no different, “ah but what about Long COVID?” is often the response. “Long COVID is no joke” they say. “It’s extremely debilitating, why risk it?” is another common response, while wearing a piece of dirty cloth over their face and bumping elbows instead of shaking hands because they irrationally believe those things are the way to avoid the plague.
Amazingly though, just like coughs and sniffles are not new and didn’t suddenly strike us down in early 2020, neither is the idea of long term effects from an illness. It used to be called Chronic Fatigue Syndrome (CFS), often diagnosed as a result of what is known as “post-viral fatigue”. There are other diagnoses it used to come labelled as. Sometimes it was ME (Myalgic Encephalomyelitis) and more recently Fibromyalgia. The problems with these diseases/syndromes are that there seems to be a massive divide in the opinions of medical professionals as to whether they are real, psychosomatic, or just not correct diagnoses.
I am not making a judgement on anyone who has/had diagnoses of either ME, Fibromyalgia or CFS, many of those people are obviously unwell with something. It is noteworthy though, that it is quite convenient for the medical profession to be able to assign arbitrary labels that appear to simply describe a nebulous set of symptoms and tell people to just deal with it. The idea that there might be some collection of causative agents that are not connected to the standard medical models of viruses/bacteria and have this pill or that injection to fix you means that doctors who are nowadays just admins and sales reps for pharmaceutical companies have little to no interest (generally, there are of course exceptions) in looking at possible environmental, dietary or other factors.
The purpose of this article is not to debate the topic of CFS itself, but to look at a French study conducted recently about the latest version of it, the much hyped “Long COVID”. Interestingly it is able to prove that the “belief you had COVID” is much more likely to result it all the “long term symptoms”, i.e. “long COVID” than actually having it, based on serology testing and the existence of antibodies. That seems weird though, right? Only thinking you had COVID when you probably just had a “cold” gives you “long COVID”, but actually having antibodies that are assumed to be the result of an actual COVID infection means you’re unlikely to end up with “long COVID”. Let’s take a look and see how this is possible.
The introduction section of the study describes the basic premise:
After infection by SARS-CoV-2, both hospitalized and nonhospitalized patients have an increased risk of various persistent physical symptoms that may impair their quality of life, such as fatigue, breathlessness, or impaired attention. Although the term “long COVID” has been coined to describe these symptoms and putative mechanisms have been proposed, the symptoms may not emanate from SARS-CoV-2 infection per se but instead may be ascribed to SARS-CoV-2 despite having other causes. In this study, we examined the association of self-reported COVID-19 infection and of serology test results with persistent physical symptoms. We hypothesized that the belief in having been infected with SARS-CoV-2 would be associated with persistent symptoms while controlling for actual infection.
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2785832
The hypothesis that “the belief in having been infected with SARS-CoV-2 would be associated with persistent symptoms” regardless of actual infection is what they are trying to establish here. It seems that there are scientists out there that recognise the placebo-effect as being a real thing. This shouldn’t be a shock to anyone, as that is why proper trials are double-blinded. Let’s take a look at some of their data…
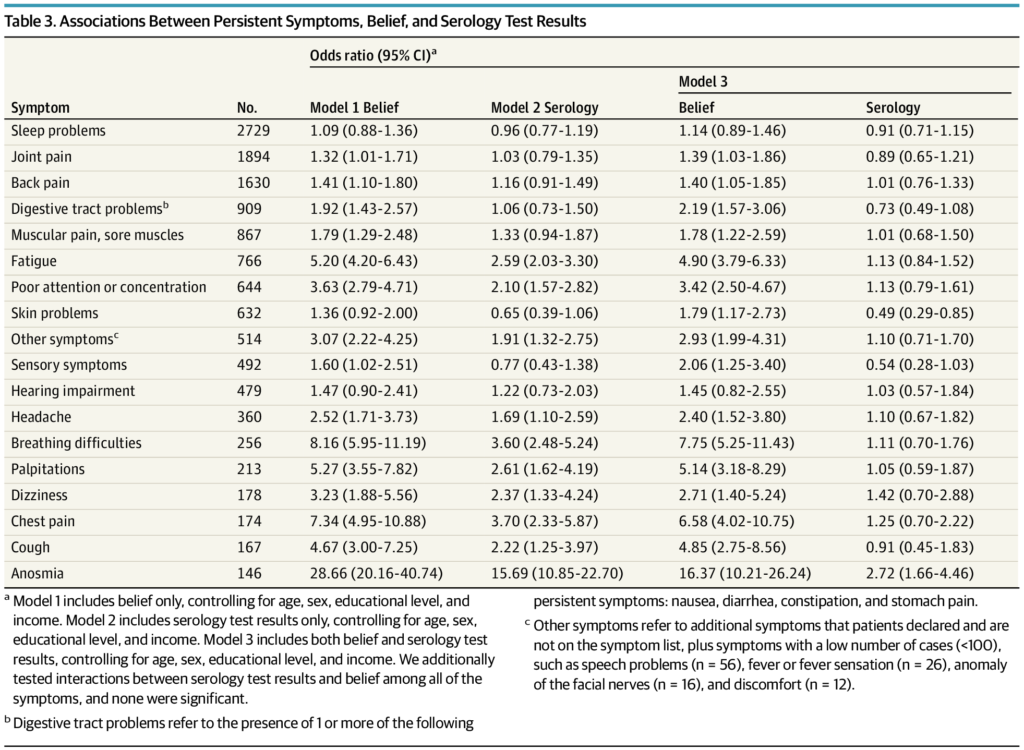
On that table, looking at model 3, which has the most compete set of regressions that measures both variables (COVID status and the belief about COVID status) and controls for variables like age, sex, income, education, etc) shows relative risk ratios. The main number should be broadly distrusted if the confidence interval (the range in brackets after) passes through 1, as that indicates you would struggle to tell it apart from being random and that the effect could have been positive or negative. The only factor that doesn’t pass through 1 using serology as a predictive variable is Anosmia, which is loss of taste/smell.
This means that losing your sense of taste/smell which is a symptom of some respiratory aliments, which is noticeable and specific is the only symptom in that list meaningfully predicted by serologically evidenced infection of what we’re told is COVID. Nothing else does. Those people were ill with something.
Side note: This article and the referenced study does not evidence the existence of the disease COVID-19, but for the purposes of this discussion, whatever some people have been ill with that gets detected serologically as COVID-19 is what is being referred to.
Now if we look at “belief that you had COVID” data in that table the values are much higher and most do not pass through 1. In almost all cases, it is 2-5 times as impactful and can be separated from chance. This is the literally the very definition of either psychosomatic disease, or conditions being ascribed to the wrong causes.
At any given time there are people who are generally unwell, and many are issues with unknown origins or causes. There is a natural tendency to want to explain them as “oh there’s lots of X going around” type of diagnoses, mostly of exclusion and arbitrary attribution that don’t have any founding in reality. Before early 2020 these people would have Chronic Fatigue Syndrome. Now it’s “Long COVID”. I’m not saying all these people are not ill, but they mostly don’t have Long COVID. They believe they do, because Governments and the media have turned Long COVID into the monster under the bed. It’s not real, but people are afraid of it because they believe it is real, and this clever study demonstrates the power of belief on people’s health, and also how having a “belief” aspect to trials generally would probably be a very informative addition.
As was already mentioned, the placebo effect is incredibly real, and it works both ways. If you believe you’re going to recover fully from an illness, you often do. If you believe you’ve got some long-term debilitating symptoms, you’ll probably have them.
Of course people do get ill, and some people will unfortunately die, but if you live in fear, as the Government wants you to, you will be more ill. Stress and fear are well known as predictors of poor health and shorter lifespans.
That study demonstrates in no uncertain terms how belief in Long COVID matters way more than actual clinical evidence of disease. You’d be hard pressed to identify actual Long COVID from that data, but imagined Long COVID is evidenced in spades.
Given that Long COVID is an often resorted to crutch for the narrative supporting masks, social distancing and of course the COVID injections (and by extension “vaccine” passports) this study sledgehammers another gaping hole in that narrative.